Today’s post comes from Ximena Ramos Salas, PhD, who is the Director of Research & Policy with Obesity Canada.
Many people have asked why we decided to update the Canadian clinical practice guidelines for the management of obesity in adults. To be honest, there were many reasons. But one of the key reasons for updating them was that the first guidelines were published in 2006 and a lot has changed in terms of our scientific understanding of obesity.
Furthermore, our research indicates that there are significant care gaps for people living with obesity as well as pervasive weight bias across healthcare, education and policy, which is leading to an increased progression of the disease at the population level.
Weight bias and obesity stigma have also created a situation where people living with obesity are marginalized and stigmatized, which is increasing health and social inequities at the population level.
What are clinical practice guidelines?
To put it simply, clinical practice guidelines summarize the current scientific and expert knowledge and provide practical recommendations for daily healthcare practice.
When we started the process of creating the new Canadian Adult Obesity Clinical Practice Guidelines, our vision was:
“To develop a non-biased, scientifically valid and trustworthy set of clinical practice guidelines with specific recommendations on the management of obesity to inform clinical decision-making that is patient-centered and to support shared decision-making in order to optimize patient care.”
With this vision in place, we started this three-year long process of creating new guidelines in collaboration with researchers, clinicians, and people living with obesity.
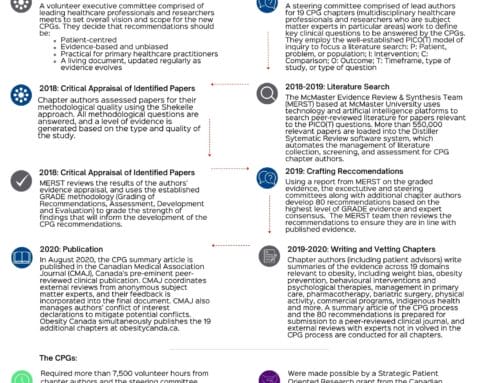
It is important to understand that the recommendations in the new clinical practice guidelines were developed systematically using a transparent procedure that included an objective evaluation of scientific evidence (quantitative and qualitative) as well as assessments and opinions of obesity experts (i.e. consensus based). A full description of the guideline development process is included in the methods section.
To be clear, clinical practice guidelines are not fixed protocols, nor are they legally binding. Instead, they are intended to serve as a guide for health care providers with the understanding that clinical discretion should always be used.
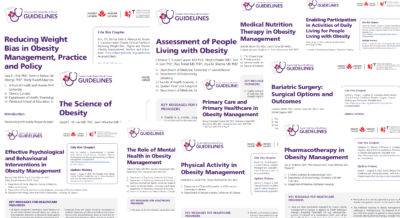
What’s new in the Canadian Adult Obesity Clinical Practice Guidelines?
At the start of the guideline development process, we recognized that there are significant misconceptions about obesity, its causes, measurement, and impacts on health. These misconceptions drive weight bias and stigma, which can be significant barriers to access to care for people living with obesity.
A key issue we wanted to address upfront, is that the traditional anthropometric-based obesity definition (BMI, weight, waist circumference) has caused confusion among clinicians, policy makers and the public.
We decided that a more comprehensive definition is needed to address obesity misconceptions and to better guide clinical care.
This is why in the new Canadian Adult Obesity Clinical Practice Guidelines we define obesity as “a chronic disease characterized by excessive or abnormal body fat that impairs health”.
As we explain in the guidelines, there are many reasons why an anthropometric-based definition of obesity is not helpful.
For instance, anthropometric measures such as BMI tell us more about a person’s body size rather than the impact of obesity on a person’s health risks.
Research also indicates that individuals can experience good health at different BMI levels and by defining obesity based on BMI alone, we may under and over diagnose individuals with obesity.
Furthermore, labeling all individuals with an elevated BMI as being “sick” may contribute to weight bias and stigma.
The reality is, however, that a significant amount of the research we reviewed to develop the guidelines is based on BMI and weight goals. This is why in the guidelines, we have called upon the obesity research community to shift this focus on BMI and weight towards health outcomes.
Research has already demonstrated that adipose tissue is a complex, heterogenous endocrine organ that secretes a variety of biologically active molecules that are important for health. Like any tissue, it can become dysfunctional and this can impact a person’s health. Future research can help shed light on why and how excess and/or abnormal adiposity impairs health.
In the meantime, based on the evidence we have now, our guidelines emphasize the need for health care providers to use existing tools and resources to assess body fat distribution and function to assess if they person has obesity or not. To be clear, it is not just the amount of body fat that matters in obesity diagnosis. At the cellular level, obesity is defined based on the pathology of adipose tissue.
We also recognize that obesity can impact health differently. For some people, obesity will have metabolic consequences, for others obesity may have mechanical consequences, for example. Therefore, we recommend that health care providers use the Edmonton Obesity Staging System to determine how obesity is impacting a person’s health before determining a treatment path.
Finally, the guidelines recommend that obesity treatment should focus on improving health, not weight loss alone. Measuring the success of obesity treatments simply based on body weight can lead to health care providers and patients missing important health benefits associated with obesity treatments. Furthermore, conceptualizing obesity treatments beyond weight loss and towards improvements in health and patient centred goals is consistent with chronic disease management principles. Chronic disease management is about improving health!
When it comes to obesity treatments, the guidelines highlight the fact that different individuals will need different treatments. There is no treatment that will work for everyone. Selecting a treatment must be done in collaboration with the patient, address root causes of obesity, and focus on achieving improved health.
So, to summarize, the new clinical practice guidelines provide a more pragmatic obesity definition to guide clinical care. This definition reflects the current scientific understanding of the homeostatic and pathological mechanisms underlying the development and maintenance of obesity and its effect on health.
Ultimately, what we hope to achieve by creating these guidelines is “to improve the standard of care, and access to, care for individuals living with obesity in all regions of Canada”. But this will depend on how Canada implements the guidelines!
The bottom line for Obesity Canada is that people with obesity deserve to have evidence-based care that is contextualized to their own realities and experiences. Healthcare professionals should support patients “where they are at”, listening to their concerns, and finding ways to support them in their own journey to health.
For years, people with obesity and those who live in large bodies have been shamed and blamed for their weight and have received inadequate care (not just obesity care but healthcare in general). Through these guidelines, we hope to change that.
As we state in the guidelines, we do not believe that everyone who has a large body or elevated weight has obesity and needs to have obesity treatment. Nor do we want to impose obesity treatment on those individuals who have been diagnosed with obesity and do not want treatment.
Obesity Canada will continue to advocate for better obesity treatments and care. But, even though many patients living with obesity ask us which treatments we endorse we will never endorse a particular treatment. This is because we know that obesity treatments must be individualized.
As a patient, you have the right to select the treatment that works for you without judgment. Our job is to make sure that you are aware of the evidence behind each treatment so that you can make an informed decision in collaboration with your healthcare provider.
Obesity research continues to evolve and the clinical practice guidelines will be updated as new research emerges. We hope new research will also continue to inform new treatment options. It is clear that current treatment options available in Canada are not enough. Rest assured, that we will continue to advocate for more research and for better treatments as well.
We believe that all Canadians regardless of their body size, weight, shape or illness deserve to receive adequate care.